

Turning down brain noise with a giant magnet (and a video mockup of my perception)
What over a dozen sessions of magnetic brain stimulation taught me about breaking a pattern that doesn't want to break

I walked into a clinic a few months ago with a brain EEG, a stack of relevant studies, and a hypothesis that most neurologists have already politely waved away. I wanted to aim an inhibitory magnetic coil at my right temporoparietal junction (rTPJ) and see if we could quiet the compensatory chaos that’s been running my cortex ragged for years.
Before I get to what happened next, if you want to understand what I’m trying to fix, watch this. But full warning: it’s uncomfortable to see and hear. Volume up for full tinnitus effect. I mocked up a 4-second simulation of what my vision and hearing actually feels like at night, capturing the visual distortion/errors, light sensitivity, and tinnitus frequency. This is just a few seconds of my daily perceptual reality.
My sensory reality — press play with caution
A few months earlier, I was in Vancouver doing that EEG — a full map of my brainwave activity. A healthy brain runs with alpha oscillations at rest. That frequency is the brain’s idle hum, keeping everything in sync. In mine, the alpha was sometimes there, but suppressed; theta, a lower frequency, was present instead.
The map showed exactly which regions were misfiring. The clinic said they’d create a custom protocol, and, for a moment, I was thrilled. For the first time in years, someone had looked at the actual electrical signature of my brain and said we can work with this.
A few months later, the Vancouver clinic sent me an email: the clinic was closing. “Really!? Now…!?” I wondered what I'd done to deserve the timing.
But I didn’t linger there. I sent the EEG and a bunch of studies to another clinic. After all, now I had the map. That measurement had to be worth something.
One clinic didn’t wave me away. They looked at the EEG, read the studies, and set up the coil. I don’t know if you can appreciate how rare it is for a clinician to investigate a mapped hypothesis and say let’s find out. Of course, I should also say that the protocol is slow, reversible, and therefore has a high safety profile. If something feels off, we pause or change the strategy.
Without them, I’d have been on a plane to Vancouver or some other city to run essentially the same experiment at several times the cost. Assuming, of course, I could find another willing clinic, and I’ve been trying for years. Without even a guarantee it would nudge things along.
The protocol, for anyone who is curious, looks like this:
one hertz, inhibitory, standard figure-8 coil
110% motor threshold
No neuronavigation with fMRI— we’re navigating by landmarks rather than brain-GPS (the Utah clinic I paid thousands for declined to send me my own brain map; I was deeply unimpressed)
Twice weekly at first; ramping to three and sometimes four per week.
I tracked everything in a detailed spreadsheet: tinnitus volume and lateralization, cognitive fog, visual distortion, autonomic symptoms, energy, mood, and when benefits appeared or faded.
Fifteen sessions so far between March and May 2026. I’ll boil down the science again and then explain what happened.
The premise
The theory is that my thalamus (at the top of the brainstem) is stuck firing at a pathological theta (slow-ish wave) rhythm when it should be in alpha (normal resting wave). My EEG shows the expected cortical signature of this. Excess theta power across the temporal, parietal, and occipital regions, with weak and disorganized alpha — the thalamic generator underneath is locked in the wrong rhythm. The TCD model predicts that this pathological theta also recruits gamma (super fast) activity at the boundaries of the affected zones to compensate, though that coupling isn’t directly visible on a standard EEG.
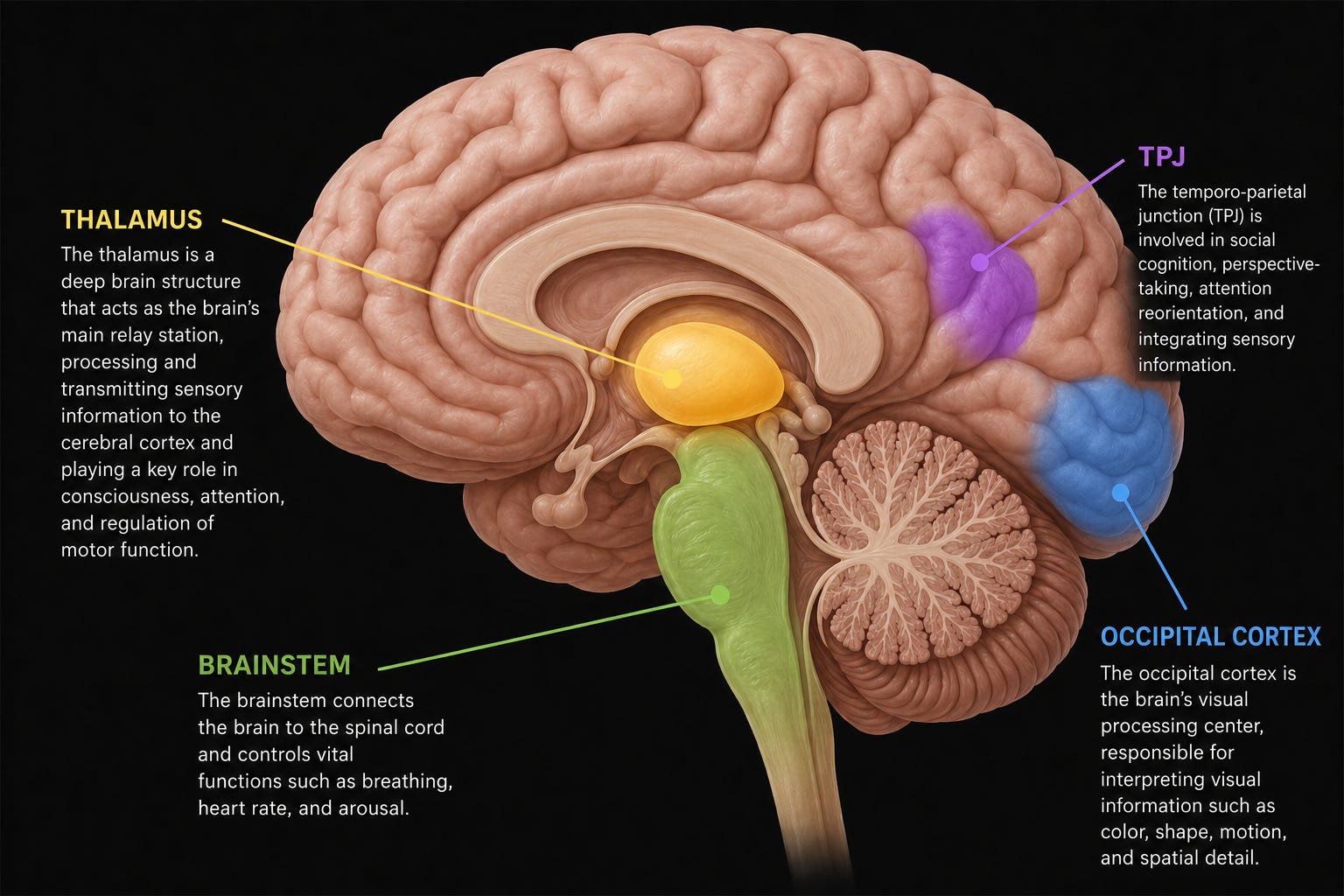
Inhibitory rTMS at 1 Hz doesn’t necessarily target a specific frequency; it reduces overall excitability at the stimulation site, disrupting the pathological oscillation so the circuit has a chance to reset (ideally, into alpha). That is, as long as there’s no damage to the infrastructure. The rTPJ was chosen because it sits at the crossroads of where my tinnitus, visual, and somatospatial processing errors converge — the busiest intersection in my dysfunctional network — and because it’s the target used in the only published case of successful rTMS treatment for visual disturbances (Creton et al., 2024).1
The magnet is essentially a part-time traffic cop, suppressing the most dysfunctional node in the loop so the circuit can find its way back to a normal rhythm (alpha). Have a look at the chart below.
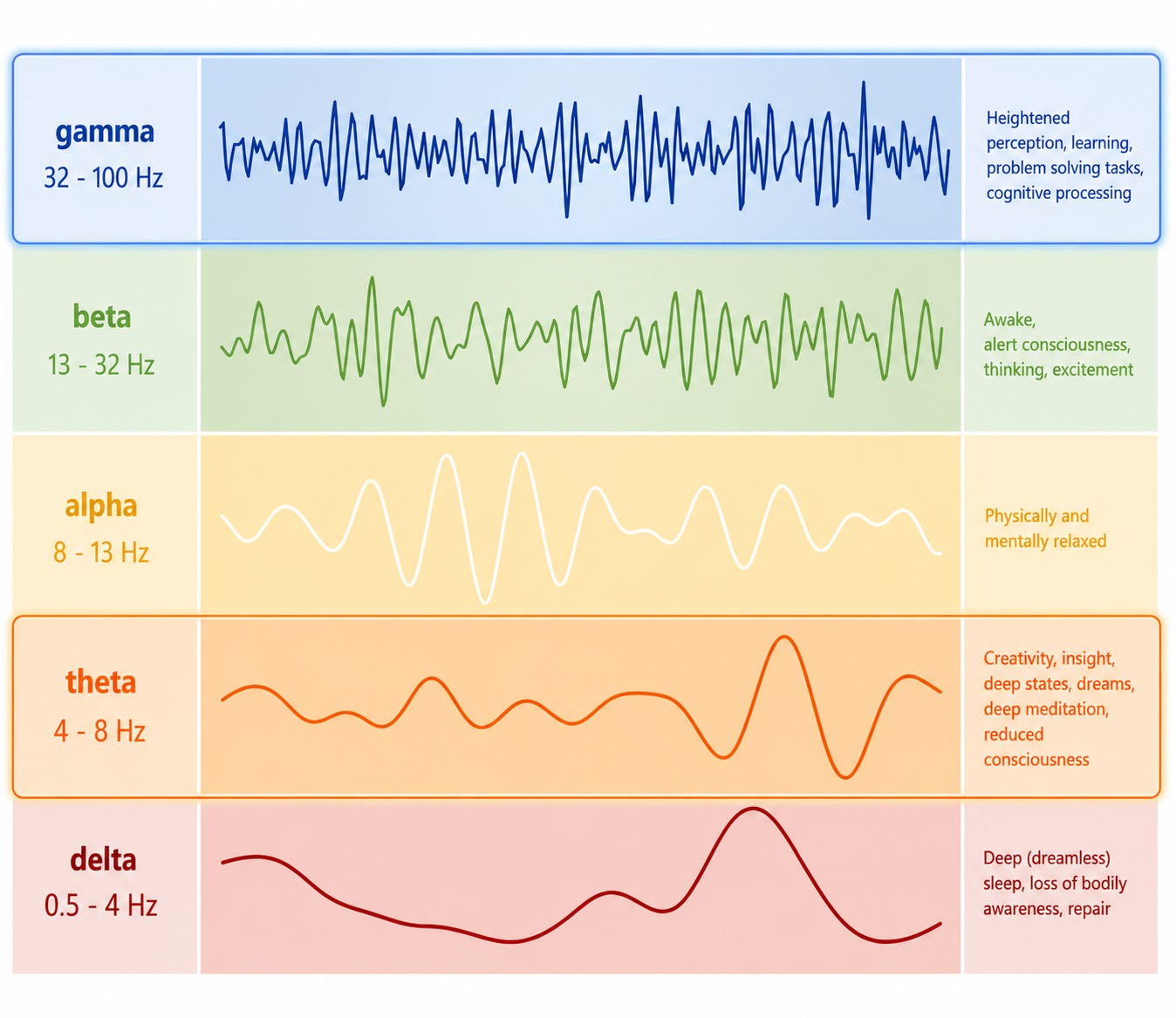
Comically, I’m in a simultaneous state of reduced consciousness and heightened perception — as you can read on the side panel — which sounds exactly appropriate.
Getting started
I showed up and was met by a staff member who had been piecing all of this together over several weeks. She was curious, polite, and seemed determined to get it right. After their detailed analysis, we were ready. I sat down in the chair. It was familiar from a protocol years earlier, though the last time I’d been in it my system was in serious overdrive and bracing for impact. This time, it was nothing.
The procedure itself doesn’t really feel like much. A light buzzing on the top of your head, like someone tapping a tuning fork against your skull. We had a great conversation, the twenty minutes passed quickly, and I went home looking forward to coming back later that week to see what the effects would be.
The effects showed up immediately. Within minutes of the first pulses, I felt tingling in my left foot — the opposite side — which is exactly what you’d expect if the magnetic field was rattling networks through the thalamocortical loop. Something was happening.
The tinnitus destabilized and felt qualitatively different. It shifted from its usual right-dominant hellfire hiss to something bilateral and shimmery. The change was refreshing, but unlikely to hold.
It didn’t.
Then, later that evening, I experienced two moments where reality itself just… stopped. It’s as if I had disappeared for a few seconds and reemerged. I gasped when I came back to life. It was shocking — a visit from an old acquaintance who used to visit me routinely. But it was transient and never came back.
rTMS was evidently knocking on the right door. Alpha was being welcomed in again, but I couldn’t get it to stay.
Brief windows of normalcy
Over the next several sessions, a pattern emerged. After each treatment, there was a window ranging from hours to days where things would improve. Tinnitus softened to a bilateral shimmer and my HR would spike and then settle. Compare that with the sound you heard above and you’ll understand the relief.
But almost every morning after, the window closed — if not completely, then at least somewhat. The old pattern came back.
Most interestingly for me, several sessions in, my eyes and ears started disagreeing. This pattern seems to suggest that parts of the network are not acting uniformly. The ear circuits were consistently improving (and snapping back) but the eye circuits were briefly worsening. The brightness and contrast both came up as light aggressively pressed into my psyche.
I wondered why would the visual cortex run hot while the auditory circuits calm down?
I have two theories:
Theory 1: Visual circuits somehow absorb the extra bandwidth. When you inhibit the rTPJ, you can relieve some pressure at the target, but the visual loop runs through a different pathway (specifically, the lateral geniculate nucleus) to the occipital cortex. As the rTPJ absorbs less, the thalamus’s chaotic energy just goes through another pipe.
Theory 2: Structural damage. The other theory is that there is interneuron damage somewhere, which means the structure won’t bear the traffic rerouting. As I’ve muddled through in various posts, cortical inhibition requires functioning GABAergic interneurons that act as the brain’s traffic controllers. They receive serotonergic input via 5-HT receptors and keep neurons from firing out of turn. They’re the reason a healthy visual cortex can process a bright room without it becoming an assault (feel grateful for this!). When serotonergic input to these interneurons is not functional, they lose their supervisory authority. The neurons start firing without adequate inhibition and the cortex runs hot.
Interestingly, a 2021 study that used TMS to suppress the primary visual cortex in visual snow patients found that the hyperexcitability didn’t originate there at all. The authors pointed instead to higher-order areas including the TPJ itself.2 This outcome raises the possibility that neither theory fully explains the visual worsening. The rTPJ may simply be closer to the visual problem, and inhibiting it may be temporarily destabilizing a node that was compensating for the visual system too.
One way or another, when the rTPJ inhibition reroutes thalamocortical traffic, the visual cortex doesn’t have the ability to handle the displaced load. It’s either (a) picking up the extra traffic; (b) has broken traffic lights; or (c) is just temporarily destabilized.
Building blocks and exhaustion
In order to spur faster recovery and address theory 2 (structural damage) I added cerebrolysin — a neurotrophic peptide — in addition to my ongoing use of other BDNF enhancers. That would be a big 5ml injection into my buttocks every morning. The idea is that it might help to rebuild some of the infrastructure by providing the building blocks for new streets and traffic lights. [Disclaimer: I’m injecting myself with this because I have little to lose, don’t do it, etc. :)]
And then, after many sessions in a row, I overcook the brain. When I do a few in a row, the old injury pattern emerges. I lose feeling on my left side, my visual “gain” spikes, my motor coordination becomes jolted and shaky, and my heartrate won’t settle. Thankfully, it’s always been transient, but those days and hours are exhausting.
Other times, like today, I achieve a wave of deep parasympathetic calm. Such a rare treat for this theta-gamma coupled guy.
The plateau’s begged question: rotating sites?
Here’s what I keep questioning. If the systemic oscillation involves theta-locked neurons projecting to multiple gamma sites simultaneously, then inhibiting one site at a time may never generate enough perturbation to destabilize the whole structure. It’s like I’m pulling one stake out of a tent that has 3. The tent wobbles, but it doesn’t collapse.
Of course, I’m not certain about this but the ongoing results beg the question. Auditory and somatosensory circuits respond to rTPJ inhibition, but visual circuits only achieve clarity, not “gain” reduction. The site of the gain — maybe the lateral geniculate nucleus — may be compensating harder. The disturbing motor effects on my left side also confirm the perturbation is reaching deep into the network. So why not the gain?
Could weekly rotation of treatment sites — rTPJ for one block, then something visual, then back to rTPJ — test whether destabilizing one anchor changes the response at another? After a block of rTPJ sessions, tinnitus bilateralizes and vision briefly clarifies; when sessions pause, the circuit snaps back and the motor sluggishness seems to flip sides. The clarity disappears. This suggests the network was (1) pushed into a new configuration; (2) started hunting for its old one; and then (3) maybe overshoots the correction on the way back.
There’s a case to try the lingual gyrus, which is a structure on the inner surface of the occipital lobe that shows hypermetabolism on PET in visual snow patients (Eren et al., 2021). It sits at the cortical end of a different loop, running through the lateral geniculate nucleus rather than through the rTPJ. But recent evidence suggests that the visual dysfunction traces back to higher-order cortical processing, not the primary or secondary visual cortex at all. Which brings us back to the rTPJ. That site may already be closer to the source than a dedicated visual target!
Which brings us back to the protocol we’re deeply into now. If destabilizing the rTPJ changes how the occipital pathway responds, at least with clarity if not in terms of brightness and contrast, that's also evidence the whole tent can perhaps come down. One peg intervention does actually destabilize the others.
My clinician rightly notes that mixing sites within a single session makes the attribution of change impossible. But weekly blocks, with clean tracking, could briefly give us a better sense of TCD’s architecture while testing the hypothesis in a controlled way.
Where to go next
For personal management, I’ve refined a lot over the back-to-back sessions as my schedule allows. I pre-dose anti-inflammatories to keep my mast cells from protesting, I run cerebrolysin concurrently, and I have recovery windows over weekends. The between-session baseline has been rising over the last several weeks, but only just.
Whether the network can be loosened from more than one direction at once is hard to say — we’ll likely try at some point. If we do, the lingual gyrus is the leading candidate.3 But I'm not sure the second peg needs loosening. It might just be where the broken gain shows up, not where it originates.
Today’s a good day. I feel tired as hell, ready to sleep at the drop of a pin, but the ease is enjoyable. The body sometimes knows how to rest, but I’m still thirsting for the brain to let it stay.
This is the third post in a series on thalamocortical dysrhythmia and its treatment. The first, “Restoring the Brain’s Tempo,” introduced the hypothesis and the search for a practitioner. The second, “Autonomic Matters of the Heart,” described the body-wide autonomic fallout.
Creton S, Boulanger G, Pereon T, Batail JM, Drapier D. (2024). “Treatment of Hallucinogen-Persisting Perception Disorder: A case report on repetitive transcranial magnetic stimulation targeting the right temporoparietal junction.” Brain Stimulation, 17(1), 107-108.
Eren et al. (2021). “Magnetic Suppression of Perceptual Accuracy Is Not Reduced in Visual Snow Syndrome.” Frontiers in Neurology, 12:658857.
Grande RB, et al. (2023). 'Repetitive TMS pilot trial for visual snow syndrome: Adverse event report.' Brain Stimulation, 16(4).